A World Day for Keratoconus
Blog vol 6.18. A World Day for Keratoconus
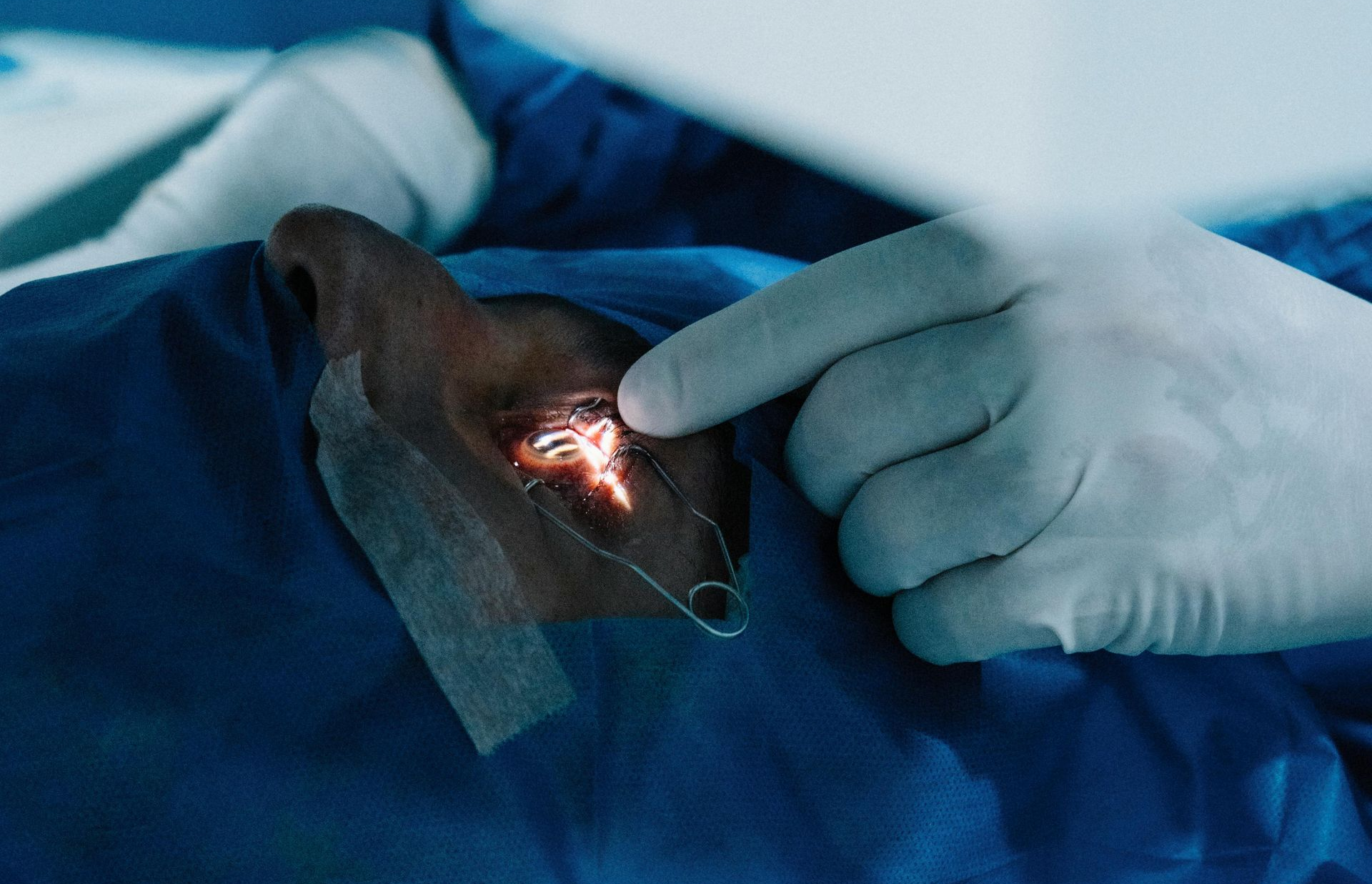
Monday of this week, in case you missed it, was World Keratoconus Day. Keratoconus, or KC for short, is an eye condition that results from having a very thin cornea. The inner pressure of the eye causes the cornea, in the front of the eye, to bulge forward and change the shape from a dome to a cone.
The condition is progressive, and if left untreated, can result ultimately in loss of the eye, pretty serious. When I first started in optometry, we fit hard contact lenses to help correct major refractive changes in KC patients. Meanwhile the condition could progress, and if the patient developed KC in their teens, they had a whole lifetime to deal with it. If things got real bad, we would have the patient go for a corneal transplant, a very drastic procedure.
In the late 1970’s, two ophthalmologists, Drs. Fleming and Reynolds, came up with the idea of using a corneal implant to change the cornea’s curvature and correct refraction in normal healthy eyes. In 1999, these intrastromal corneal ring segments (INTACS) were approved for correcting mild myopia.
As always, the earth and world did not stand still, and we started using lasers to reshape the corneal stroma. Today this procedure, called LASIK, is the procedure of choice for most myopia corrections. The INTACS procedure, though a viable option, is more invasive than LASIK, so not desirable for a healthy eye, however, it is very helpful in the treatment of keratoconus. Dr. Joseph Colin used two segments of PMMA (a hard contact lens material) for the ring implant and was able to help low to moderate risk KC patients who could not tolerate contact lens correction. INTACS provided a correction to the refraction and allowed everyday function for the patient.
The world did not stand still again, and now there is a procedure called corneal cross-linking, where the eye is saturated with riboflavin and bombarded with ultraviolet light creating “300 year old” corneas and strengthening the collagen bonds, thus slowing down and even halting the progress of KC. Awesome, all we have to do is catch the KC before it progresses and harden the cornea so it doesn’t change. So we now put all children on a corneal mapping device that screens for KC and we are right as rain.
In a perfect world, yes, but… there are a lot of people who were not diagnosed early and KC has done permanent damage. Even if you strengthen the cornea with cross-linking, it doesn’t fix the shape of the cornea and there will still be residual refractive changes. The treatment of choice for refractive problems in KC patients, INTACS, has been improved and is now called Corneal Allogenic Intrastromal Ring Segment, CAIRS for short. Instead of a PMMA ring implant, a donor corneal stroma is used which is more compliant with the host, and allows for a wider pool of candidates to receive the segment. It is also more customizable during the procedure with improved outcomes. The end result is less glare sensitivity, discomfort and scarring, and a better refractive result than INTACS. The procedure is safe to use on KC patients who have received cross-linking and can also help other corneal conditions like Pellucid’s Marginal Degeneration and is safe for high risk KC patients. (Read more here CAIRS Gaining Momentum - Issuu). CAIRS is about 10 years old and here to stay.
Did you know that lime green or chartreuse ribbons are worn to increase KC awareness?
‘til next week (year),
The good doctor





